Evaluation of an Ovarian Cystic Mass: A Clinical Guide for Accurate Diagnosis
Ovarian cystic masses are commonly encountered in gynecologic practice and imaging studies. While most ovarian cysts are benign and self-limiting, some may represent significant pathology, including malignancy. A structured, evidence-based evaluation is essential to distinguish benign conditions from those requiring urgent intervention.
This article outlines a practical, step-by-step approach to the evaluation of an ovarian cystic mass, integrating clinical assessment, imaging findings, risk stratification, and management principles.
What Is an Ovarian Cystic Mass?
An ovarian cystic mass refers to a fluid-filled or partially fluid-filled lesion arising from the ovary. These masses may be:
- Physiologic (e.g., follicular or corpus luteum cysts)
- Benign neoplastic (e.g., serous cystadenoma, dermoid cyst)
- Pathologic or malignant
Correct evaluation depends heavily on patient age, menopausal status, and imaging characteristics.
Step 1: Clinical Assessment
Key History Elements
- Age and menopausal status (premenopausal vs postmenopausal)
- Pelvic pain, bloating, abdominal distension
- Acute symptoms suggesting torsion or rupture
- Menstrual irregularities or abnormal uterine bleeding
- Pregnancy status
- Personal or family history of ovarian or breast cancer
- Use of hormonal therapy or fertility treatment
Physical Examination
- Adnexal mass size and mobility
- Tenderness
- Presence of ascites
- Nodularity or fixation (concerning for malignancy)
Step 2: Imaging Evaluation (First-Line Investigation)
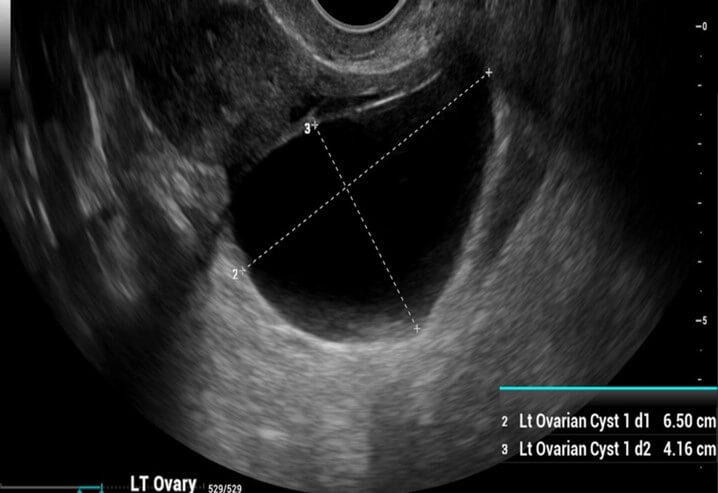
Transvaginal Ultrasound (TVUS)
Transvaginal ultrasound is the gold standard initial imaging modality for evaluating ovarian cystic masses.
×
![]()
Benign Ultrasound Features
- Unilocular cyst
- Thin, smooth walls
- Anechoic (clear fluid)
- No solid components
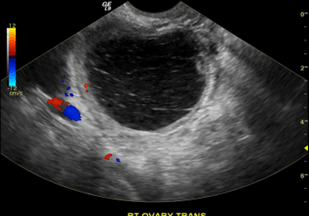
- No internal blood flow on Doppler
Suspicious or Malignant Features
- Solid areas or papillary projections
- Thick septations (3 mm)
- Irregular cyst walls
- Internal vascularity
- Ascites
- Bilateral ovarian masses
Common Ultrasound Patterns
- Hemorrhagic cyst: Reticular or lace-like internal echoes
- Endometrioma: Homogeneous "ground-glass" appearance
- Dermoid cyst (mature teratoma): Echogenic areas with acoustic shadowing
Step 3: Risk Stratification Systems
To standardize evaluation and reduce unnecessary surgery, several validated tools are used:
- IOTA Simple Rules
- O-RADS (Ovarian-Adnexal Reporting and Data System)
- Risk of Malignancy Index (RMI)
- Combines ultrasound score, menopausal status, and CA-125 level
These tools help determine the need for observation, further imaging, or surgical referral.
Step 4: Tumor Markers (Adjunctive Role)
Tumor markers should be used selectively and interpreted cautiously.
Commonly Used Markers
- CA-125
- Most useful in postmenopausal women
- Can be elevated in benign conditions such as endometriosis, fibroids, or pelvic inflammatory disease
In Younger Patients (if malignancy suspected)
- Alpha-fetoprotein (AFP)
- Beta-hCG
- Lactate dehydrogenase (LDH)
- Inhibin (for suspected sex-cord stromal tumors)
Step 5: Special Clinical Scenarios
Ovarian Cysts in Pregnancy
- Most are functional and resolve spontaneously
- Surgical intervention is reserved for:
- Persistent cysts > 5-6 cm
- Suspicious imaging features
- Complications (torsion, rupture)
Acute Pelvic Pain
- Consider
- Ovarian torsion
- Cyst rupture
- Hemorrhage
- These conditions may require emergency surgical management.
Step 6: Management Principles
| Clinical Scenario |
Recommended Management |
| Simple cyst <5 cm (premenopausal) |
Observation |
| Simple cyst 5–7 cm |
Repeat ultrasound |
| Simple cyst >7 cm |
MRI or surgical evaluation |
| Complex or suspicious cyst |
Referral to gynecologic oncology |
| Postmenopausal cyst with solid features |
Surgical evaluation |
Red Flags Requiring Urgent Referral
- Postmenopausal status
- Ascites
- Elevated CA-125
- Solid components on imaging
- Rapid growth
- Fixed or nodular mass
Conclusion
The evaluation of an ovarian cystic mass requires a systematic approach that integrates clinical context, high-quality ultrasound imaging, and risk stratification tools. Most ovarian cysts are benign, but early identification of suspicious features is critical for optimal outcomes.
Timely referral and appropriate follow-up can prevent unnecessary interventions while ensuring early detection of malignancy when present.